All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know ALL.
The ALL Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the ALL Hub cannot guarantee the accuracy of translated content. The ALL Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The ALL Hub is an independent medical education platform, sponsored by Amgen and Autolus. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View ALL content recommended for you
Obecabtagene autoleucel (obe-cel) for relapsed/refractory B-ALL: The FELIX study
 José María Ribera
José María Ribera Wendy Stock
Wendy Stock André Baruchel
André Baruchel Nicolas Boissel
Nicolas Boissel Daniel DeAngelo
Daniel DeAngeloDo you know... Which of the following is a predictor of improved long-term outcomes following treatment with obe-cel for adults with R/R B-ALL?
During the ALL Hub Steering Committee meeting in April 2026, Daniel DeAngelo chaired a discussion on the latest findings from the phase Ib/II FELIX trial (NCT04404660) investigating obecabtagene autoleucel (obe-cel), a CD19-directed chimeric antigen receptor (CAR) T-cell therapy in adults with relapsed/refractory (R/R) B-cell acute lymphoblastic leukemia (B-ALL).1 The discussion featured contributions from Ibrahim Aldoss, José María Ribera, André Baruchel, Wendy Stock and Nicolas Boissel.
Obecabtagene autoleucel (obe-cel) for relapsed/refractory B-ALL: The FELIX study
In his presentation, DeAngelo outlined the currently approved CD19-directed CAR T-cell therapies for the treatment of B-ALL, including obe-cel and brexucabtagene autoleucel (brexu-cel) for adults with R/R B-ALL, and tisagenlecleucel (tisa-cel) for paediatric and young adult patients with R/R B-ALL.2–7 He then discussed the key findings from the phase Ib/II FELIX trial (Figure 1), including long-term outcomes and predictors of response to obe-cel, in adults with R/R CD19-positive B-ALL (Figure 2).1,8-10
Figure 1. FELIX study design*
.png)
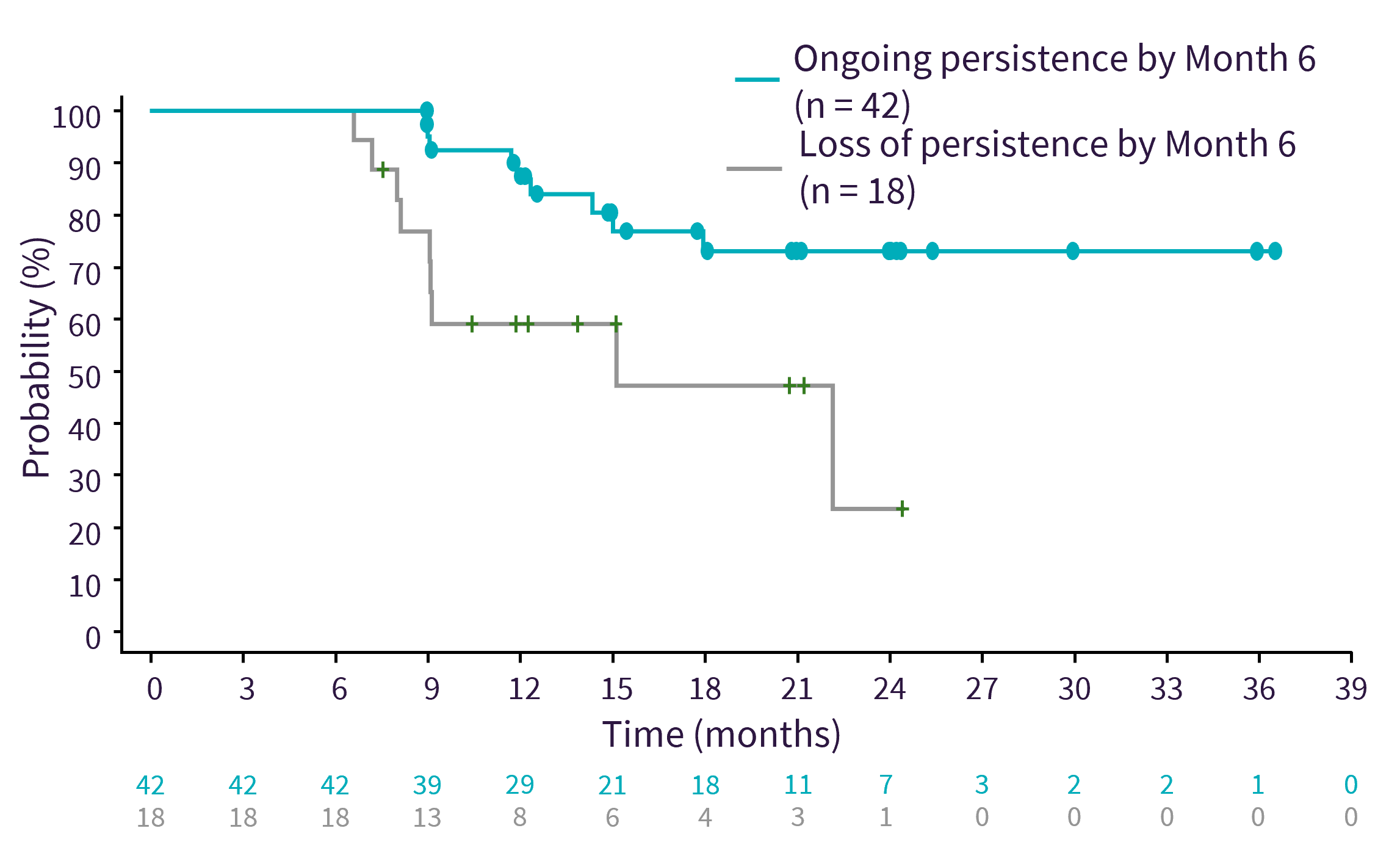
Figure 2. Ongoing CAR T-cell persistence correlates with long-term EFS*
Key points
- The FELIX trial demonstrated that obe-cel produces high remission rates, durable responses, and a favourable safety profile in patients with R/R B-ALL, with outcomes linked to lower disease burden at lymphodepletion and sustained CAR T-cell persistence.1
- After a median follow-up of 32.8 months (range, 19.9–52.8 months), 38.4% of responders remained in remission without stem cell transplant or other non-protocol specified therapies.9
- These findings suggest that some patients may not require additional therapy; however, longer follow-up, further analyses, and independent validation are needed to confirm these results.9
- Lower disease burden at lymphodepletion and ongoing CAR T-cell persistence were independent factors associated with long-term remission and survival.
- Patients with ≤20% bone marrow blasts had an overall response rate of 85%, compared with 73% in patients with >20% bone marrow blasts. 9
- Patients with ongoing CAR T-cell persistence had a prolonged predicted event-free survival compared with patients with a loss of CAR T-cell persistence at Month 12 or at Month 6.8
- Age did not appear to adversely affect outcomes, with comparable event-free survival and overall survival observed in patients aged <55 years and ≥55 years; rates of Grade ≥3 cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS remained low across age groups.11
- Ongoing phase II clinical studies are investigating obe-cel in different ALL settings, including:
- As consolidation therapy for adults with newly diagnosed high-risk B-ALL (NCT07053059)12
- As consolidation therapy in adults with ALL in first complete remission without measurable residual disease (NCT07400029)13
- In pediatric patients with R/R B-ALL (NCT06173518); preliminary findings from the phase Ib/II CATULUS study (NCT06173518) have shown promising efficacy and a favorable safety profile of obe-cel in pediatric patients with R/R B-ALL14,15
- Real-world data from the ROCCA consortium (40 North American centers) supported the findings from the FELIX trial, with high response rates that were similar between patients treated with brexu-cel (n = 53) and obe-cel (n = 36);16 real-world evidence is still accumulating following the relatively recent approval of obe-cel.
- Despite the durable long-term responses observed with obe-cel, the role of stem cell transplant consolidation in patients with R/R ALL remains to be fully established.
- Current practice remains variable and the optimal sequencing of CAR T-cell therapy and allogeneic hematopoietic stem cell transplantation remains to be defined through longer-term, prospective data.
- Additionally, there is currently uncertainty regarding the optimal intensity of pre-CAR T-cell cytoreduction in patients with high blast counts, reflecting a need to balance achieving deeper disease control against avoiding delays to CAR T-cell infusion.
- Data from the FELIX trial indicates that lower disease burden is associated with improved outcomes.8
- Furthermore, optimization of infection prophylaxis, monitoring, and management is required in patients undergoing CAR T-cell therapy, given the high infection risk associated with prior intensive therapies, bridging regimens, and prolonged cytopenias.
- Overall, the FELIX study established obe-cel as an effective CD19-directed CAR T-cell therapy for adults with R/R B-ALL, demonstrating high remission rates, durable responses, low rates of severe CRS and ICANS, and encouraging long-term outcomes, particularly in patients with low disease burden and sustained CAR T-cell persistence.
This educational resource is independently supported by Autolus. All content is developed by SES in collaboration with an expert steering committee. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content

.jpeg&w=3840&q=75)
.webp&w=3840&q=75)