All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know ALL.
The ALL Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the ALL Hub cannot guarantee the accuracy of translated content. The ALL Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The ALL Hub is an independent medical education platform, sponsored by Amgen and Autolus. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View ALL content recommended for you
Strategies to prevent relapse post HSCT / cellular therapy in B-ALL
Featured:
 Charles Mullighan
Charles Mullighan José María Ribera
José María Ribera Wendy Stock
Wendy Stock Anita Rijneveld
Anita Rijneveld Sabina Chiaretti
Sabina Chiaretti André Baruchel
André Baruchel Ibrahim T. Aldoss
Ibrahim T. Aldoss Daniel DeAngelo
Daniel DeAngeloDo you know... Multiple factors influence the risk of relapse and guide the decision to initiate maintenance therapy after allo-HSCT. What factor is NOT associated with higher rates of relapse?
During the ALL Hub Steering Committee meeting in November 2025, key opinion leaders met to discuss strategies to prevent relapse post hematopoietic stem cell transplantation (HSCT) or cellular therapy in B-cell acute lymphoblastic leukemia (B-ALL). The meeting opened with a presentation by Ibrahim Aldoss and featured a discussion including Charles Mullighan, José María Ribera, Sabina Chiaretti, André Baruchel, Wendy Stock, Daniel DeAngelo, and Anita Rijneveld.
Strategies to prevent relapse post HSCT / cellular therapy in B-ALL
Strategies to prevent relapse post HSCT / cellular therapy in B-ALL
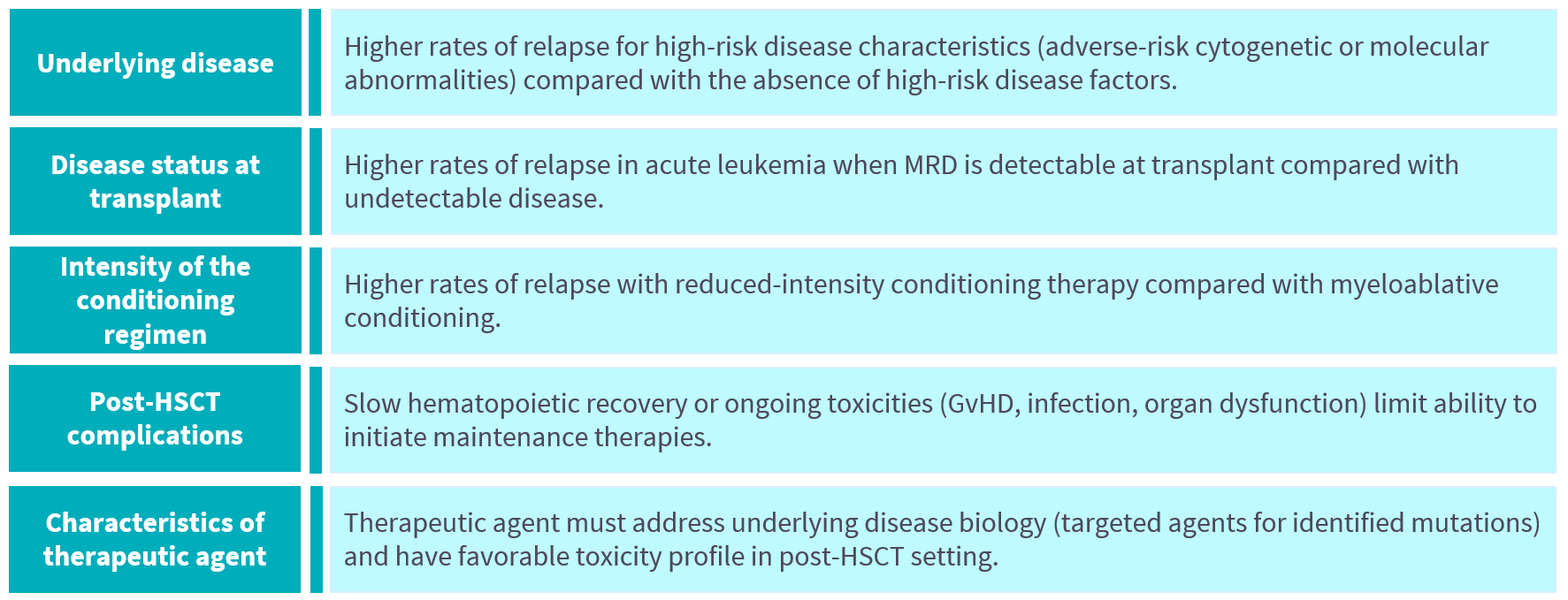
During his presentation, Aldoss highlighted that despite advances in multi-agent chemotherapy and novel immunotherapies enabling an increased number of patients to undergo allogeneic (allo)-HSCT – a potentially curative approach in B-ALL – post-transplant relapse, as well as relapse following CAR T-cell therapy, remains a major cause of treatment failure.1 He discussed several studies exploring relapse-preventive measures post‑transplantation (Figure 1), including established strategies such as tyrosine kinase (TKI) maintenance in patients with Philadelphia-chromosome positive (Ph+) ALL. He shared clinical study data for newer strategies, such as the use of blinatumomab, inotuzumab ozogamicin, or prophylactic donor-derived CAR T-cell therapy, which have shown promising initial activity in patients with B-ALL.1 Aldoss also outlined the major considerations that influence the decision to initiate maintenance therapy after allo-HSCT or salvage therapy post-CAR T-cell therapy (Figure 2).2
Figure 1. Strategies to prevent relapse post allo-HSCT in ALL*
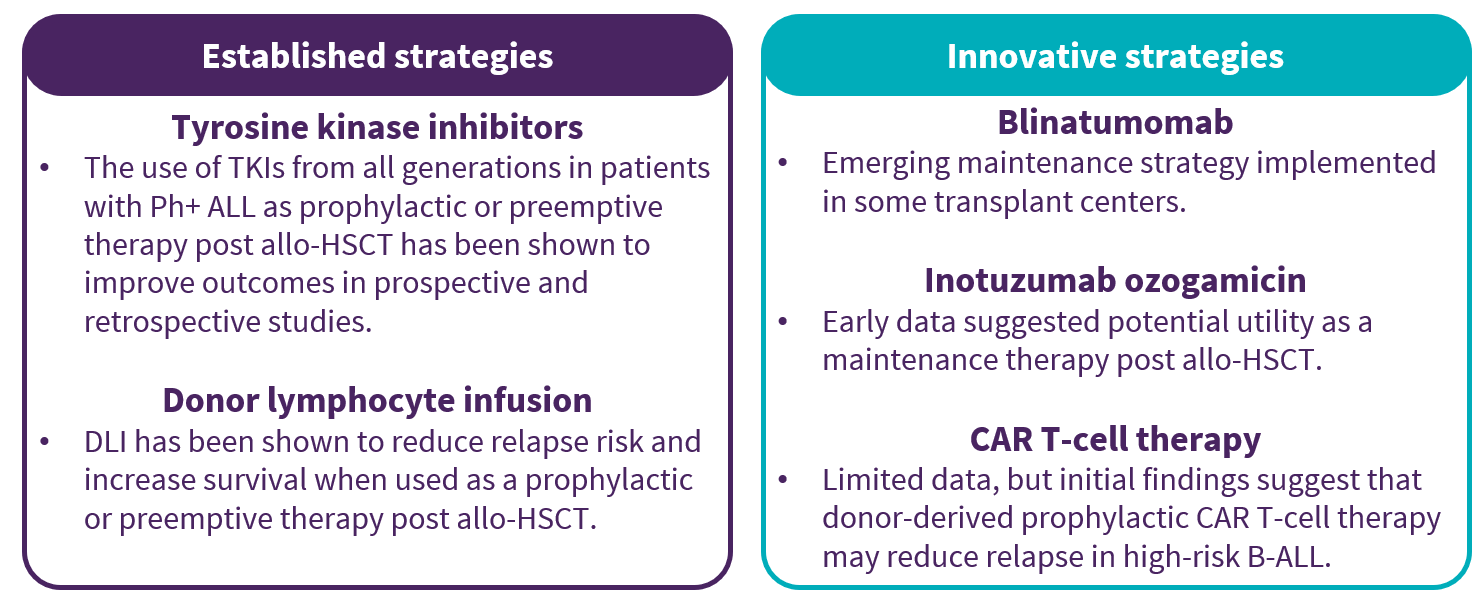
Figure 2. Considerations for maintenance therapy initiation*
Key points
- Despite advances in novel strategies for the treatment of B-ALL, post-transplant relapse remains a major cause of treatment failure.3
- Multiple factors influence relapse risk and can be used to guide maintenance therapy decisions.1 These include underlying disease characteristics (e.g. high-risk), measurable residual disease (MRD) status at transplant, intensity of the conditioning regimen, post-HSCT complications and the characteristics of the therapeutic agent to address the underlying disease biology.1,2
- A study evaluating the prognostic value of next-generation sequencing-based MRD in 158 adult patients with B-ALL/T-cell ALL undergoing HSCT found that the detection of pre-transplant MRD and post-transplant MRD was associated with an increased risk of relapse.4
- For patients undergoing allo-HSCT or CAR T-cell therapy, MRD assessment should be performed before allo-HSCT or CAR T-cell therapy (for patients in hematologic remission) and approximately every 2–3 months for at least the first year after allo-HSCT or CAR T-cell therapy.5
- There are several established and innovative strategies being explored as preventive measures post‑transplantation.1
- Established therapies, such as TKI maintenance in patients with Philadelphia-chromosome positive (Ph+) ALL, have been shown to reduce the risk of relapse.1,6-9
- In a retrospective study of 473 patients with de novo Ph+ ALL who underwent allo-HSCT, 157 patients received TKI after allo-HSCT.6 In the post-transplant period, prophylactic TKI was a significant factor for improved leukemia-free survival (hazard ratio [HR], 0.44; p = 0.002) and overall survival (HR, 0.42; p = 0.004), and a lower relapse incidence (HR, 0.40; p = 0.01).6
- Several studies have shown that preemptive or prophylactic donor lymphocyte infusion (DLI) post-transplantation, guided by MRD status or loss of chimerism, may prevent overt relapse in patients with B-ALL.1,10-13
- To address the risk of graft-versus-host disease (GvHD) post DLI, a pilot study showed that a repetitive schedule of low-dose DLIs every 2 months for at least 36 months reduced both relapse and GvHD rates in patients with high-risk ALL (n = 11) post allo-HSCT.13
- Newer strategies, including the use of blinatumomab, inotuzumab ozogamicin, or prophylactic donor-derived CAR T-cell therapy, in patients with B-ALL have shown promising initial activity.1,14-16
- Blinatumomab: A phase II trial (NCT02807883) showed that blinatumomab maintenance therapy after allo-HSCT was feasible, with a manageable safety profile, in 21 patients with high-risk B-ALL.14
- Inotuzumab ozogamicin: A phase I trial (NCT03104491) assessed the safety and efficacy of low-dose inotuzumab ozogamicin maintenance therapy after allo-HSCT in 18 patients with high-risk ALL.15 Low-dose inotuzumab ozogamicin maintenance therapy after allo-HSCT had a favorable safety profile, with no incidence of sinusoidal obstruction syndrome.15
- Prophylactic donor-derived CAR T-cell therapy: A study investigated the use of prophylactic donor-derived CAR T-cell infusion after allo-HSCT in 23 patients with high-risk B-ALL.16 When compared with a contemporary cohort of 44 patients with high-risk B-ALL who did not receive post-transplant maintenance therapy, patients who received prophylactic donor-derived CAR T-cell infusion had reduced relapse rates.16
- To prevent relapse following CD19 CAR T-cell therapy in patients with B-ALL, current strategies focus on modifying pre-infusion risk factors, enhancing CAR T-cell persistence, and optimizing consolidation strategies to extend durable remissions.3
- Intervention strategies include preemptive consolidative HSCT, re-infusion with CAR T-cells, administering T-cell antigen-presenting cells following CAR T-cell therapy, treatment with full human or humanized CAR T-cells and the development of next-generation CAR T cells to target more than one antigen.3
- In patients who relapse post CAR T-cell therapy, the relapse phenotype can inform salvage strategies.3 For example, treatment options for patients with a relapse phenotype of CD19 negative ALL include chemotherapy, CD22-targeted therapies (inotuzumab ozogamicin) or experimental therapies such as B-cell activating factor-receptor (BAFF-R) CAR.3
- Further studies are needed to determine the optimal strategies to prevent relapse post allo-HSCT and for salvage therapy following CAR T-cell therapy.1
This educational resource is independently supported by Pfizer. All content was developed by SES in collaboration with an expert steering committee. Funders were allowed no influence on the content of this resource.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content

