All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know ALL.
The ALL Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the ALL Hub cannot guarantee the accuracy of translated content. The ALL Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The ALL Hub is an independent medical education platform, sponsored by Amgen and Autolus. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View ALL content recommended for you
Optimizing asparaginase use in AYA patients: Key recommendations from the ASH 2026 guidelines for first-line management of ALL
Do you know... When do the ASH 2026 guidelines recommend switching from pegaspargase to an Erwinia based formulation?
Treating acute lymphoblastic leukemia (ALL) in adolescent and young adult (AYA) patients, typically defined as 15–39 years old, has long been challenging.1 Although pediatric and adult treatment protocols are well established, AYA patients have historically fallen into a therapeutic ‘gray area’ with differing approaches favored by pediatric and adult specialists.1
Over the past decade, evidence has shown that pediatric-inspired, asparaginase-based regimens improve outcomes in AYA patients compared with conventional adult therapy.1 This shift has been reflected in updates from the National Comprehensive Cancer Network and European LeukemiaNet.2–7 However, concerns have persisted about higher rates of asparaginase-associated toxicity in AYA patients compared with younger children and, until now, there has been a lack of guidance tailored specifically to this population.
The American Society of Hematology (ASH) 2026 guidelines for first-line management of ALL in AYA patients provide the first age-specific recommendations and strongly endorse pediatric-inspired, asparaginase-based therapy.1 This article summarizes the key asparaginase-related recommendations, the evidence and rationale underpinning them, and practical guidance for optimizing treatment.
Figure 1. ASH 2026 guidelines for first-line management of ALL in AYA patients*
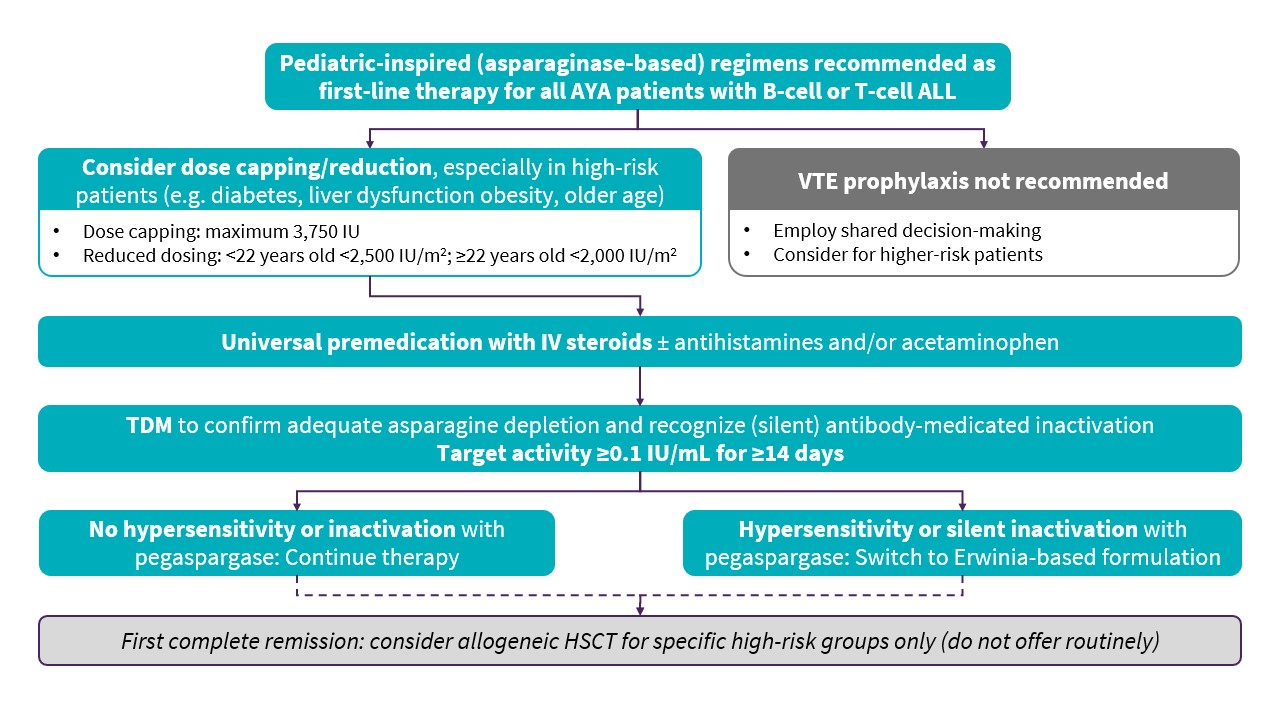
Asparaginase-based regimens as first-line therapy1
The guidelines make a strong recommendation for pediatric-inspired, asparaginase-containing regimens for all AYA patients with newly diagnosed B-cell or T-cell ALL. In this context, pediatric-inspired regimens include intensive asparaginase exposure, whereas adult-style regimens use less intensive asparaginase or omit it entirely. This recommendation is based on substantial and clinically meaningful survival benefits consistently demonstrated with pediatric-inspired regimens, and the multidisciplinary panel reached unanimous agreement on this point.
Toxicity, a longstanding concern in AYA patients receiving asparaginase, was also considered. The panel concluded that available evidence does not show a significant difference in overall toxicity between pediatric-inspired and adult-style regimens and, in fact, in relation to treatment-related mortality, the evidence favors pediatric-inspired regimens.
Treatment burden is always a consideration in ALL, not least for AYA patients, who have distinctive care needs and social risk factors and for whom long, arduous regimens can have a significant impact on productivity and job revenue. In making this recommendation the panel considered that, while implementation of pediatric-inspired regimens does require additional resources and infrastructure, there are also burdens associated with adult-inspired regimens. Overall, the panel felt that any differences in treatment burden were difficult to quantify and were outweighed by the clear survival advantage of pediatric-inspired regimens.
This is a strong recommendation with moderate certainty of evidence. Although randomized controlled trials are limited, the panel considered the large body of comparative studies consistently favoring pediatric-inspired regimens to provide compelling support.
Asparaginase dosing1
Although the panel considered pediatric-inspired and adult-style regimens to be similar in terms of overall toxicity in AYA patients, they suggest using empiric dose capping and dose reductions to help mitigate asparaginase-related adverse events.
- Dose capping: Maximum pegaspargase dose of 3,750 IU
- Reduced dosing:
- In patients <22 years old, weight-based dose <2,500 IU/m2
- In patients ≥22 years old, weight-based dose <2,000 IU/m2
These approaches may be particularly appropriate for AYA patients with risk factors such as diabetes, obesity, older age, or underlying liver disease.
This recommendation reflects evidence suggesting that dose capping or reduction may offer some toxicity benefit without compromising remission or survival outcomes. It is a conditional recommendation based on very low certainty of evidence.
Prophylactic premedication as standard1
The ASH 2026 guidelines make a strong recommendation for universal prophylactic premedication for all AYA patients receiving first-line asparaginase-containing regimens. This recommendation represents a shift from selective premedication and reinforces the central role of asparaginase in the guideline.
As a minimum, premedication should include intravenous steroids, with antihistamines and/or acetaminophen added as appropriate. Therapeutic drug monitoring (TDM) should be used alongside premedication to detect silent inactivation that may be masked by premedication.
Beyond the individual patient benefit or preventing hypersensitivity reactions, premedication may also help reduce healthcare costs. Evidence shows that premedication reduces both the incidence of hypersensitivity reactions and the need to switch to Erwinia-based formulations, potentially reducing reaction-related hospital admissions, switching costs, and additional clinic visits for administration of Erwinia-based formulations.
Therapeutic drug monitoring1
Specific recommendations are made on the use of TDM in the context of dose capping/reduction and premedication. For patients receiving capped or reduced doses, TDM is advised as good practice to confirm adequate asparagine depletion.
In the context of premedication, TDM should be used to:
- Determine whether hypersensitivity reactions are associated with antibody-mediated inactivation.
- Identify silent inactivation, which may be masked by premedication.
Given the heterogeneity of available evidence, the guidelines recommend targeting activity levels ≥0.1 IU/mL for ≥14 days to ensure adequate asparagine depletion.
Switching to alternative asparaginase formulations1
In cases of hypersensitivity to PEG-asparaginase, including silent inactivation detected through TDM, the guidelines make a strong recommendation to switch to an Erwinia-based formulation rather than discontinue asparaginase therapy. This recommendation reflects the importance of maintaining adequate asparaginase exposure; evidence shows that missed doses are associated with poorer survival and higher relapse risk. Although the panel acknowledged the potential drawbacks of switching, including increased cost and resource use, it concluded that the benefits for disease control and survival outweigh these considerations.
Due to lack of evidence, no recommendation was made regarding the relative benefits of desensitization vs switching to an alternative asparaginase formulation. Similarly, the panel were unable to make a recommendation on resuming (or changing) asparaginase therapy following a non-hypersensitivity toxicity. Clinicians are instead encouraged to consult other treatment protocols, product monographs, and guidance documents.
VTE prophylaxis1
The guidelines also address venous thromboembolism (VTE) prophylaxis, another area of uncertainty in AYA patients with ALL treated with first-line asparaginase-containing regimens. Routine prophylaxis with cryoprecipitate replacement (or fibrinogen concentrate) or unfractionated heparin is not recommended, on the basis that these interventions may be associated with greater harm than benefit.
Considering prophylaxis with low-molecular-weight heparin, direct-acting oral anticoagulants, and antithrombin replacement, the panel made no recommendation, based on insufficient evidence. However, the guidelines encourage individualized shared decision-making and consideration of VTE prophylaxis for higher risk patients.
Conclusion1
The ASH 2026 guidelines mark a pivotal moment in the care of AYA patients with ALL, providing the first specific guidance for this population. Together, these recommendations offer a clearer, more consistent framework for delivering intensive, curative therapy to AYA patients – a population that has historically faced fragmented approaches and variable outcomes.
The new guidelines emphasize the central role of pediatric-inspired asparaginase-based regimens for first-line therapy, and provide guidance on practical measures such as universal premedication, TDM, and timely switching to Erwinia-based formulations. While the guidelines highlight further evidence needs, including prevention and treatment of asparaginase toxicity and the comparative effects of desensitization/rechallenge vs switching asparaginase formulations, these recommendations should support clinicians to optimize first-line therapy, thereby improving outcomes for AYA patients with both B-cell and T-cell ALL.
This educational resource is independently supported by Jazz Pharmaceuticals. All content was developed by SES in collaboration with an expert steering committee. Funders were allowed no influence on the content of this resource.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content

.jpeg&w=3840&q=75)
